

A 61-year-old female patient came to us after consultations and rejections from several medical institutions near her place of residence and as well as in Kyiv. Prolonged jaundice, hyperthermia, and intoxication were progressively weakening and deteriorating her condition.
Upon her referral to us, in the transplantation and abdominal organ surgery department, we performed additional percutaneous transhepatic drainage of the right liver lobe. This was necessary because the left lobe had been previously drained, but it was insufficient for complete biliary decompression.
For further evaluation, we conducted: CT scans of the chest and abdominal organs, 3D modeling of the liver (CT volumetry and segmentation), CT scans of the pelvic organs. In the region of the confluence of intrahepatic bile ducts, extending to the right hepatic duct (RHD), left hepatic duct (LHD), and segment 4 duct (Sg4), a tumor measuring 23x15x23 mm was visualized. The left portal vein (LPV) was invaded, and the right lateral hepatic artery (rLHA) originated from the left gastric artery (LGA). The middle hepatic artery (MHA) had contact with the tumor, and an aneurysm up to 5 mm was present in the MHA. The right hepatic artery (RHA) showed no signs of contact with the tumor.
Preoperative diagnosis: Klatskin tumor type IV according to Bismuth-Corlette classification, cT3NxMo, stage IIIa, grade II.
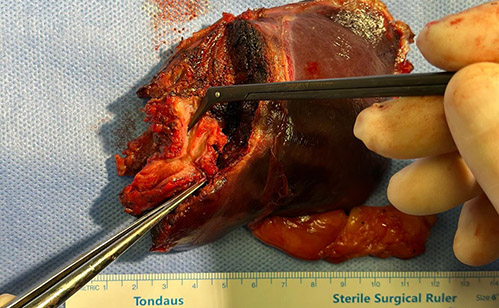
The patient underwent surgery, including left hemihepatectomy, excision of the hepaticocholedochus, caudate lobectomy, resection and reconstruction of the middle hepatic artery, D3 lymphadenectomy.
No postoperative complications were observed, and the patient was discharged for outpatient treatment on the 12th day after the intervention.


The anatomical proximity of perihilar bile ducts to vascular structures increases the risk of invasion and renders many cases inoperable. However, Mizuno et al. (2022) from Nagoya University presented one of the largest experiences with extended liver resections involving arterial and portovenous resections: 146 and 157 cases, respectively. There was no statistically significant difference in complication rates and mortality between patients with vascular resections and those without resection (48% and 50%, and 1.2% and 3.6%, respectively). However, overall survival was lower in patients who underwent vascular resection compared to those who had liver resection alone, but it was higher in patients who were not operated on at all (30, 61, and 10 months, respectively).
We extend our gratitude to the teams of the Heart Institute and Volyn Regional Clinical Hospital.
Surgical Team:
Yurii Bakunets, Mykhailo Zahriichuk, Mykola Kondratiuk, Roman Samokishchuk, Mykola Melnyk, Stepan Maruniak.